Your Guide to Wildfire Smoke Health Risks
This study guide covers the established health effects of wildfire smoke, from acute respiratory impacts to chronic disease and mortality, with a focus on the disproportionate toxicity of wildfire PM2.5 and the populations most at risk. It synthesizes key epidemiological studies and practical protective measures to help students prepare for exams in environmental health and public health.
Updated:
The Exam Answer Starts With PM2.5
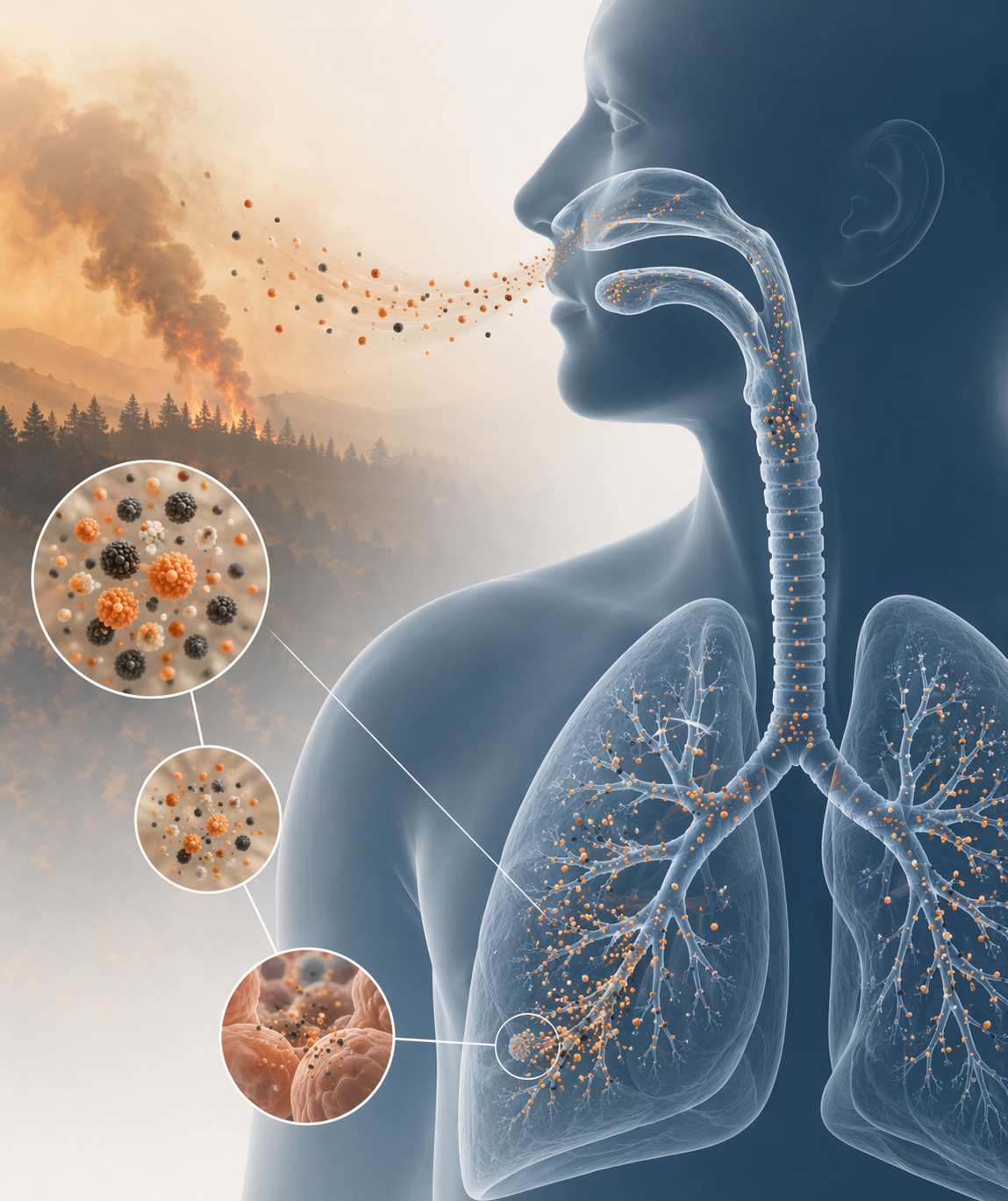
In a health risks of wildfire smoke study guide, the first point is not simply that smoke irritates the lungs. The stronger answer is that wildfire smoke is a complex exposure, fine particulate matter smaller than 2.5 micrometers in diameter is the main exam-relevant hazard, and wildfire-origin PM2.5 may cause more harm per unit mass than PM2.5 from many other ambient sources. Reid et al.’s critical review of 43 epidemiological studies found the most consistent evidence for respiratory morbidity from wildfire smoke exposure, while cardiovascular findings were growing but less consistent at the time of review [1].
That distinction matters because public-health exams often ask students to connect exposure, mechanism, outcome, and evidence strength. A vague answer such as “wildfire smoke is bad for lungs and heart” loses the part that explains why agencies and researchers track PM2.5 so closely: particles this small can penetrate deeply into the respiratory tract, reach the small airways and alveolar region, and carry a mixture of organic compounds, gases, and combustion byproducts produced by burning vegetation and built materials [1].
A useful exam sentence is: wildfire smoke PM2.5 is treated as more than generic ambient PM2.5 because its chemical composition, combustion source, and epidemiological associations suggest disproportionate respiratory toxicity. Aguilera et al. tested this directly in Southern California and found that, for the same 10 µg/m³ increase, wildfire PM2.5 was associated with 10% more respiratory emergency department visits than non-wildfire PM2.5 [2]. The important part is not only the estimate. It is that four statistical approaches pointed in the same direction, which makes the result harder to dismiss as an artifact of one modeling choice [2].
What “More Toxic Per Unit Mass” Means
When a study says wildfire PM2.5 is more toxic per unit mass, it is not saying that every wildfire plume has identical chemistry or that every exposed person will have the same response. It means that, after comparing equal mass concentrations, wildfire-attributed PM2.5 shows stronger associations with certain health outcomes than PM2.5 from other sources. In Aguilera et al., the outcome was respiratory emergency department visits, and the comparison was made per 10 µg/m³ increase [2].
This is where many short-answer responses become too broad. “PM2.5 causes inflammation” is a reasonable mechanism-level statement, but it does not separate wildfire smoke from traffic, industrial, or other ambient particle mixtures. Wildfire smoke changes with fuel type, combustion temperature, distance from the fire, atmospheric aging, and the presence of burned structures. The particle size category is the same, but the exposure mixture is not necessarily the same.
The best-supported version of the toxicity claim is therefore narrower and stronger: wildfire PM2.5 appears especially harmful for respiratory outcomes, and the evidence is reinforced when different epidemiological approaches produce similar results. Across the studies cited here, respiratory hospital admissions increased by 1.3% to 10% per 10 µg/m³ increase in wildfire PM2.5, a range that reflects different settings, populations, exposure definitions, and outcome measures rather than one universal biological constant [2].
| Exam term | What it means in this topic | Common mistake |
|---|---|---|
| Wildfire smoke | A changing mixture of fine particles, gases, and combustion products | Treating it as one uniform substance |
| PM2.5 | Fine particles small enough to reach deep lung regions | Forgetting that source and composition can modify toxicity |
| Per unit mass toxicity | Health association compared at the same PM2.5 mass concentration | Reading it as proof that every plume is equally toxic |
| Association | An epidemiological relationship between exposure and outcome | Calling every observational result direct proof of causation |
Respiratory Effects Have the Strongest Evidence
If an exam asks for the most established health effects of wildfire smoke, respiratory morbidity should come first. Reid et al. found consistent evidence linking wildfire smoke exposure with respiratory outcomes, especially asthma exacerbations, chronic obstructive pulmonary disease effects, respiratory infections or symptoms, emergency department visits, and hospital admissions [1]. This is the backbone evidence because it separates what is relatively well established from what remains more uncertain.
The causal pathway is also easier to explain for respiratory outcomes than for many longer-latency endpoints. Inhaled fine particles and irritant gases can worsen airway inflammation, trigger bronchoconstriction, reduce pulmonary function, and push people with asthma or COPD from self-management into urgent care. The epidemiological outcome then becomes visible as more rescue medication use, more clinic visits, more emergency department visits, or more hospital admissions.
Aguilera et al. strengthens this respiratory argument by showing that wildfire PM2.5 was associated with more respiratory emergency department visits than non-wildfire PM2.5 at the same mass increment [2]. For students, that finding is worth remembering because it converts a general pollution lesson into a wildfire-specific one: the exposure source can matter even when the pollutant metric looks familiar.
The practical consequence is straightforward. During smoke days, respiratory clinics, emergency departments, school nurses, and caregivers should expect symptoms to rise first among people whose airways are already reactive or compromised. That does not mean healthy adults have no risk. It means baseline vulnerability changes the probability that the same exposure becomes an urgent medical event.
Mortality Estimates Are Large, but Not Interchangeable
Mortality is the next major outcome to understand, and it needs careful handling. A Yale School of Public Health summary of Ma et al. reported an estimated 11,415 non-accidental deaths per year attributable to long-term wildfire PM2.5 exposure across the contiguous United States [3]. A separate UCLA summary of Connolly et al. reported about 52,500 to 55,700 excess deaths in California over 11 years [4]. Those numbers are both serious, but they are not measuring the same geography, time window, exposure model, or counterfactual.
The mistake is to rank these estimates as though the larger number automatically means a more dangerous place or a more definitive study. The California estimate spans 11 years and focuses on one state with repeated severe wildfire seasons [4]. The contiguous United States estimate is an annual burden estimate for long-term wildfire PM2.5 exposure across a broader geography [3]. Different exposure surfaces, statistical assumptions, and population baselines can shift the final burden estimate.
A global estimate cited in the wildfire-smoke health literature attributed roughly 339,000 premature deaths annually to landscape fire smoke, which places wildfire and biomass smoke in a much larger international burden context [1]. That estimate should be used as a scale marker, not as if it were directly comparable to a state-level California estimate or a contiguous-US estimate using different methods.
For an exam, the safest formulation is: wildfire smoke is associated with a substantial mortality burden, but mortality estimates vary by geography, population, exposure window, outcome definition, and modeling approach. That answer shows that the student understands both public-health magnitude and methodological boundaries.
Cardiovascular Findings Matter, but the Evidence Is More Mixed
Cardiovascular outcomes should not be ignored, but they should not be presented with the same confidence as respiratory morbidity. Reid et al. characterized the cardiovascular evidence as growing but not yet consistent, with some studies finding associations with outcomes such as cardiac arrest and others not finding clear effects [1]. That is an evidence-strength distinction, not a claim that the heart is irrelevant.
Biologically, cardiovascular concern is plausible. Fine particles can contribute to systemic inflammation, oxidative stress, autonomic imbalance, endothelial dysfunction, and changes in thrombosis risk. Epidemiologically, however, the signal can be harder to isolate because cardiovascular events are influenced by age, medication use, heat, baseline disease, socioeconomic factors, and short-term behavioral changes during smoke episodes.
A good answer therefore says that wildfire smoke may increase cardiovascular risk, especially among older adults and people with existing cardiovascular disease, but the evidence base has historically been less consistent than for respiratory emergency visits and hospitalizations [1]. That wording leaves room for concern without flattening the hierarchy of evidence.
Pregnancy and Birth Outcomes
Pregnant people belong in the vulnerable-population group because fetal development can be sensitive to environmental exposures and because birth outcomes have been linked to wildfire smoke timing. In the studies summarized by Holm et al., first-trimester wildfire smoke exposure was associated with 1.076 times higher odds of preterm delivery, while second-trimester exposure was linked to a 9.7 g reduction in birth weight [5].
Those numbers should be interpreted at the population level. A small average shift in birth weight does not predict an individual infant’s outcome, but across many pregnancies it can move more births toward clinically vulnerable ranges. The timing also matters: first-trimester and second-trimester associations should not be merged into one generic “pregnancy risk” sentence if the exam asks about exposure windows.
Who Is Most Vulnerable
Vulnerability is not just a list of sympathetic groups. It is risk stratification: who receives more exposure, who has less physiological reserve, who is more likely to convert exposure into disease, and who has fewer practical options for avoiding smoke.
| Group | Why risk is higher | Most relevant outcomes |
|---|---|---|
| Children | Developing lungs, higher ventilation relative to body size, outdoor activity patterns, dependence on adults for protection | Asthma symptoms, respiratory visits, school and activity disruption |
| Older adults | Higher baseline cardiopulmonary disease burden and lower physiological reserve | Emergency department visits, hospitalizations, premature mortality |
| Pregnant people | Potential fetal-development sensitivity and timing-specific exposure windows | Preterm delivery, lower birth weight |
| People with asthma, COPD, or cardiovascular disease | Lower margin before symptoms become clinically serious | Exacerbations, urgent care, hospital admissions |
| People with limited housing, filtration, transport, or healthcare access | Less ability to create clean indoor air or leave high-smoke areas | Higher cumulative exposure and delayed care |
Children are a major concern because exposure and development overlap. Holm et al. reported that about 7.4 million U.S. children are affected by wildfire smoke annually, citing Rappold et al. [5]. The number is useful because it prevents the topic from being framed as only a problem for people living immediately next to a flame front. Smoke travels, school schedules change, outdoor activity changes, and caregivers make decisions based on air quality that may shift within hours.
Older adults show the burden in a different way. An NBER summary reported that Medicare beneficiaries aged 65 and older experience about 10,070 premature deaths and 191,541 excess emergency department visits per year from wildfire smoke [6]. Those endpoints are not minor irritation; they are severe outcomes in a population with high baseline vulnerability.
People with pre-existing respiratory or cardiovascular disease should be identified because smoke exposure can worsen an already unstable baseline. Someone with controlled asthma may need rescue medication more often; someone with COPD may lose enough reserve to require urgent evaluation; someone with cardiovascular disease may face added physiological stress even if the cardiovascular epidemiology is less uniform than the respiratory evidence.
Acute Exposure Versus Longer-Term Exposure
Wildfire smoke health effects are often acute because smoke episodes produce short-term spikes in PM2.5. That is why emergency department visits, asthma exacerbations, and hospital admissions are common study outcomes. The exposure window may be same-day, lagged by several days, or measured over a smoke episode, depending on the study design.
Longer-term exposure questions are different. They ask whether repeated seasonal smoke, chronic regional exposure, or cumulative wildfire PM2.5 contributes to mortality and chronic disease burden. Ma et al.’s estimate of 11,415 annual non-accidental deaths across the contiguous United States is an example of this longer-term burden framing rather than a single-smoke-day emergency response estimate [3].
Students should keep those designs separate. Acute studies are well suited to detecting short-term spikes in symptoms, emergency visits, or hospitalizations. Long-term burden studies can estimate population-level mortality attributable to exposure, but they depend heavily on modeled exposure histories, baseline mortality rates, and assumptions about the exposure-response relationship.
How to Read a Wildfire Smoke Study
A strong exam response can often be built by checking four elements: exposure definition, outcome definition, population, and comparison. Without those, a wildfire smoke claim can sound precise while hiding major differences between studies.
- Exposure: Is the study measuring total PM2.5, wildfire-attributed PM2.5, smoke days, satellite plume presence, or modeled concentrations?
- Outcome: Is the endpoint respiratory symptoms, medication use, emergency department visits, hospital admissions, birth outcomes, or mortality?
- Population: Is the study about children, older adults, pregnant people, Medicare beneficiaries, or the general population?
- Time window: Is it same-day exposure, lagged exposure, trimester exposure, seasonal exposure, or long-term cumulative exposure?
- Comparison: Is the study comparing wildfire PM2.5 with non-wildfire PM2.5, smoke days with non-smoke days, or exposed regions with less exposed regions?
This checklist also explains why some estimates differ without one study being “wrong.” A study of pediatric asthma visits during smoke days answers a different question from a national long-term mortality model. A trimester-specific birth outcome analysis answers a different question from an all-age emergency department study. Precision in the question is part of the answer.
Protective Measures: Reduce the Dose
The prevention logic follows directly from the evidence: reduce inhaled PM2.5, protect high-risk groups early, and improve indoor air before symptoms force medical care. The CDC advises people at higher risk, including children, older adults, pregnant people, and people with heart or lung disease, to take wildfire smoke exposure seriously and reduce exposure during smoke events [7].
The most useful protective measures are not interchangeable. Staying indoors helps only if indoor air is cleaner than outdoor air. Closing windows helps only if indoor sources are controlled and filtration is available. A mask helps only if it filters fine particles and fits well enough to reduce leakage.
| Measure | What the evidence supports | Exam-ready interpretation |
|---|---|---|
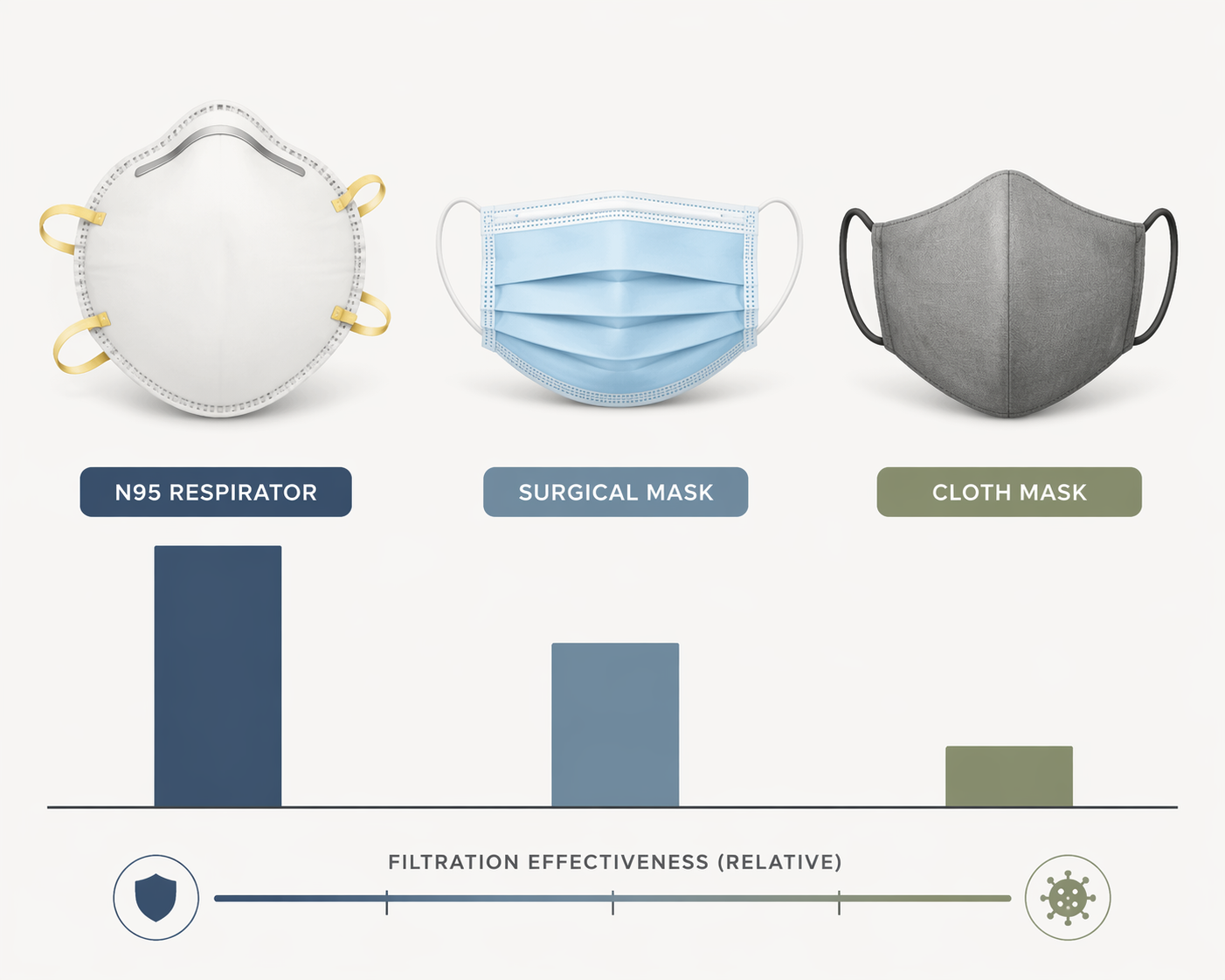
| N95 respirator | N95 respirators without fit testing reduce exposure by about 80% for children and adults | Best mask option among those listed when it fits and is worn correctly |
| Surgical mask | Surgical masks reduce exposure by about 20% | Some protection, but far less than an N95 |
| Cloth mask | Cloth masks provide inconsistent protection | Do not treat as reliable PM2.5 protection |
| HEPA filtration | HEPA air filtration can reduce indoor PM2.5 by 60% to 80% | Important indoor-air intervention, especially for high-risk households |
Holm et al. reported that N95 respirators without fit testing reduce exposure by about 80% for both children and adults, surgical masks by about 20%, and cloth masks provide inconsistent protection [5]. The difference is large enough to be worth memorizing because it changes practical advice. “Wear a mask” is too vague; mask type and fit determine whether the intervention meaningfully reduces fine-particle exposure.
Indoor filtration is the other high-yield intervention. HEPA filtration can reduce indoor PM2.5 by 60% to 80%, which makes clean-air rooms, portable HEPA units, and properly maintained HVAC filtration central tools during smoke episodes [5]. For high-risk households, that can be more realistic than evacuation and more protective than simply closing windows in a leaky building.
During a smoke event, the operational sequence is simple: check local air quality, reduce outdoor exertion, keep indoor air clean, use a well-fitting respirator when outdoor exposure cannot be avoided, and prioritize children, older adults, pregnant people, and people with cardiopulmonary disease. The evidence does not reduce wildfire smoke risk to one number. It shows a patterned public-health problem: a disproportionately toxic PM2.5 exposure produces acute respiratory morbidity, contributes to mortality and adverse birth outcomes, and falls hardest on predictable high-risk groups.
References
- Critical Review of Health Impacts of Wildfire Smoke Exposure — Environmental Health Perspectives, 2016
- Wildfire smoke impacts respiratory health more than fine particles from other sources — Nature Communications, 2021
- Long-term exposure to wildfire smoke associated with higher risk of death — Yale School of Public Health
- UCLA study finds upwards of 50,000 deaths in 11 years — UCLA Luskin
- Health effects of wildfire smoke in children: a narrative review — Journal of Exposure Science & Environmental Epidemiology, 2020
- Health Consequences of Wildfire Smoke — NBER
- How Wildfire Smoke Affects Your Body — CDC
Comments
Join the discussion with an anonymous comment.