
How to interpret enlicitide side effect data
Learn to critically evaluate drug safety data using the enlicitide CORALreef trials as a real-world example. This guide shows you how to compare adverse event rates against placebo to distinguish true safety signals from background noise.
Updated:
The first number that can make an enlicitide side effects study look alarming is 64%. In CORALreef Lipids, 64% of participants taking enlicitide had an adverse event. If that is the only number you read, the drug sounds noisy. Then the placebo arm appears: 62% had an adverse event too.[1]
That two-point difference is the beginning of the interpretation, not a detail to mention after the fact. In a trial safety table, the raw adverse event rate tells you how often something medically unfavorable was recorded after treatment started. It does not, by itself, tell you that the drug caused those events. The comparison arm is what keeps the table honest.
Enlicitide, now approved as Lipfendra, is a once-daily oral PCSK9 inhibitor for reducing LDL cholesterol in adults with hypercholesterolemia.[2] That background matters, but it is not the main skill here. The useful lesson is how to read the safety data without treating every percentage as either a warning siren or a marketing reassurance.
Start With The Placebo Comparison
CORALreef Lipids enrolled 2,909 participants and gives a clean example of why safety interpretation starts across the row, not down the drug column. The important question is not, “Did many people report something?” In a population at cardiovascular risk, over months of follow-up, many people will. The question is whether the enlicitide arm shows a pattern meaningfully different from placebo.
| Safety outcome in CORALreef Lipids | Enlicitide | Placebo | How to read it |
|---|---|---|---|
| Any adverse event | 64% | 62% | High in both arms; not a strong signal by itself |
| Serious adverse event | 10% | 12% | No excess serious-event burden with enlicitide |
| Discontinuation due to adverse events | 3% | 4% | Few participants stopped because of AEs in either arm |
| Mortality | 0.7% | 0.7% | Balanced between arms |
| New-onset diabetes | 6% | 6% | Balanced between arms |
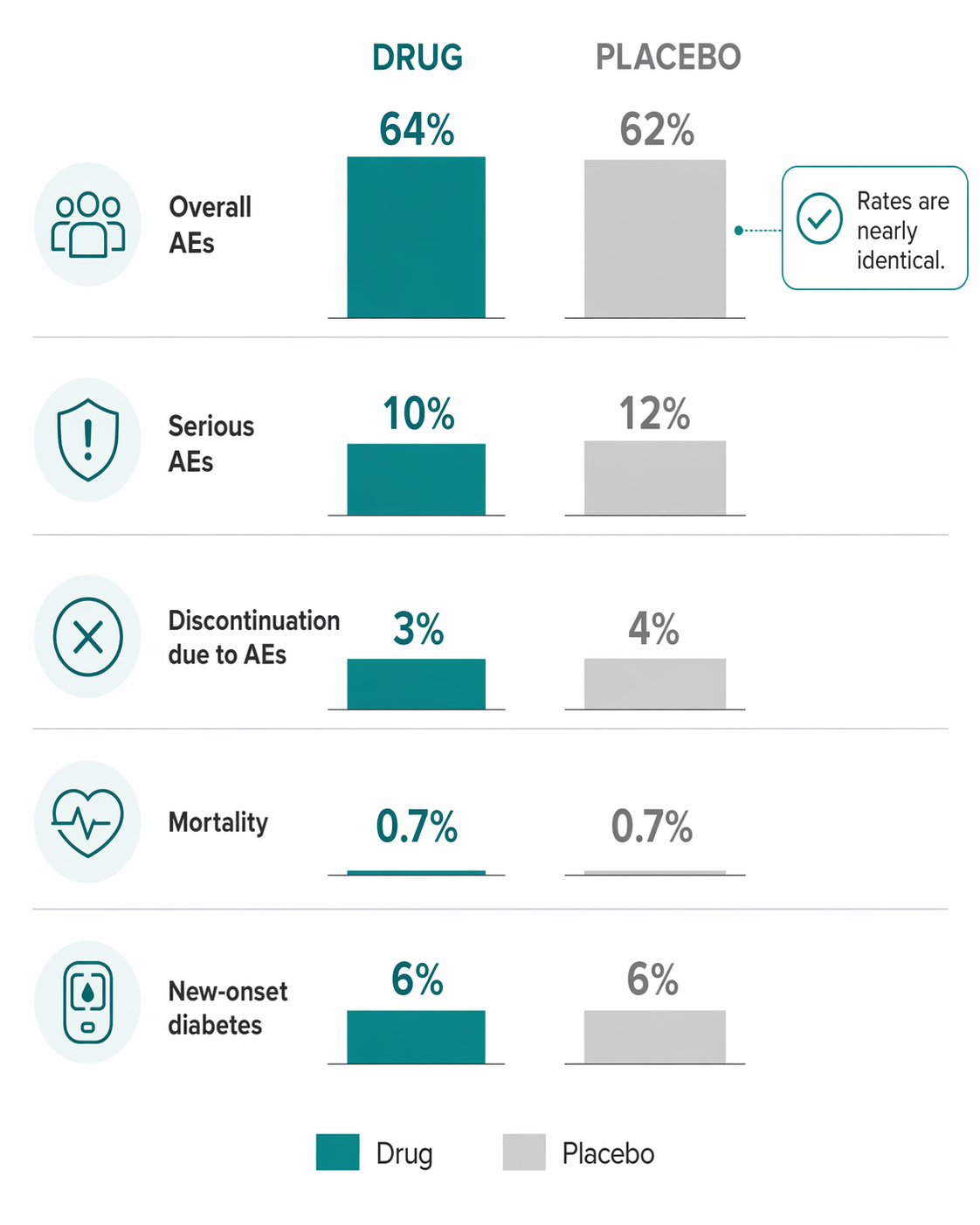
Those paired numbers are why “64% had an adverse event” is not the conclusion. It is the setup. Serious adverse events were 10% with enlicitide and 12% with placebo. Discontinuation due to adverse events was 3% with enlicitide and 4% with placebo. Mortality was 0.7% in both groups. New-onset diabetes was 6% in both groups.[1]
For a student reading this table before rounds or an exam, the disciplined sentence would be: overall adverse events were common, but comparable to placebo, and the more consequential safety outcomes did not show an excess in the enlicitide arm. That is stronger than saying the drug was “well tolerated” and more precise than saying “64% had side effects.”
What The Safety Terms Are Actually Doing
An adverse event is any unfavorable medical occurrence recorded during the trial period. It can be related to the study drug, unrelated to it, or uncertain. A participant who develops a headache, respiratory infection, fall, lab abnormality, or worsening of an existing condition may contribute to the adverse event count if it meets the trial’s reporting rules.
That is why the overall AE line tends to be broad. It is deliberately sensitive. It catches medical events first and asks causality questions later. In CORALreef Lipids, that broad net caught events in nearly two-thirds of both the enlicitide and placebo groups.[1] The similar rates make it hard to argue that the overall AE burden is being driven mainly by the drug.
A serious adverse event is a narrower and more clinically weighted category. It generally includes events such as death, life-threatening events, hospitalization, disability, congenital anomaly, or other medically important outcomes. The exact regulatory definition is more formal than that, but for reading a paper, the practical move is simple: serious AEs deserve their own comparison because they are not interchangeable with minor symptoms.
Here, the serious AE comparison does not move against enlicitide: 10% versus 12% with placebo.[1] That does not prove that no serious event was related to the drug. It does mean the trial did not show an excess serious-event rate in the enlicitide group.
Discontinuation due to adverse events answers a different question: did the event burden become intolerable enough, or concerning enough, that participants stopped treatment? In CORALreef Lipids, discontinuation due to AEs was 3% with enlicitide and 4% with placebo.[1] That is a practical tolerability clue. People can report adverse events and still continue therapy; stopping rates help separate background medical noise from events that disrupt treatment.
An adverse reaction is narrower still. It implies a suspected causal relationship to the drug. This is where the reader should become more demanding, not less. A reaction signal usually needs more than a raw count: it should show a plausible imbalance versus placebo, a pattern across related symptoms, biological plausibility, dose or timing coherence when available, or confirmation in larger data.
The HeFH Signal Is A Different Reading Problem
The specific side effects worth slowing down for did not come from treating the 64% overall AE line as frightening. They came from a smaller, distinct population: CORALreef HeFH, which enrolled 303 participants with heterozygous familial hypercholesterolemia. In that group, diarrhea occurred in 7% of enlicitide-treated participants versus 2% with placebo, and dizziness occurred in 9% versus 4%.[2]
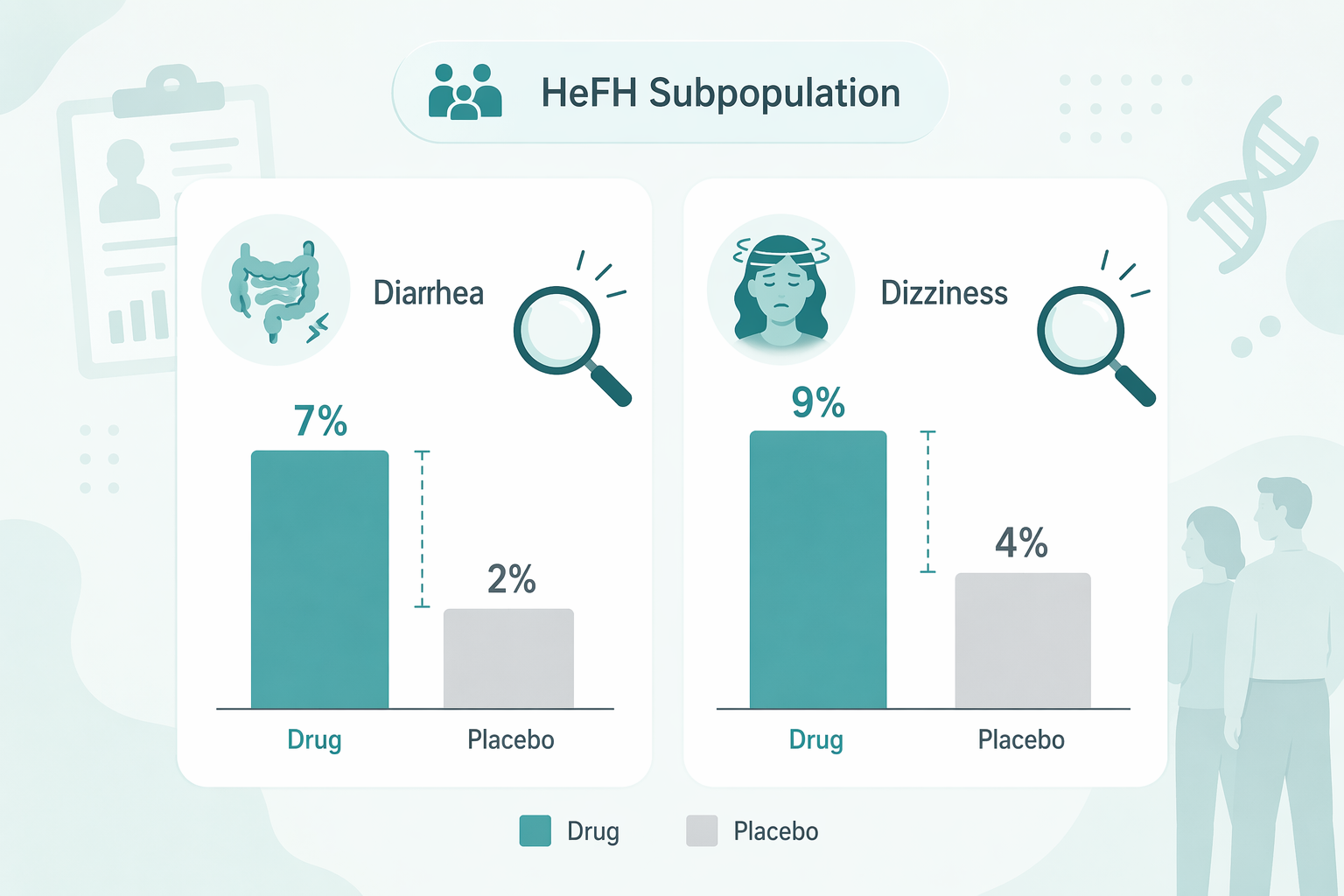
This is what a plausible treatment-emergent signal looks like in a safety table. The percentages are much smaller than 64%, but the between-arm difference is more informative. A 7% versus 2% diarrhea comparison tells you something different from a 64% versus 62% any-AE comparison. The first points toward a symptom imbalance. The second mostly tells you that recorded medical events were common in both randomized groups.
The population distinction matters. The diarrhea and dizziness figures come from the HeFH trial, not from the larger CORALreef Lipids safety table. The broader trial did not present a standout imbalanced adverse event in the same way. Combining the two as if they were one undifferentiated dataset would make the interpretation look cleaner than the evidence allows.
A careful clinical interpretation can therefore hold both points at once: the larger placebo-controlled dataset is reassuring on overall AEs, serious AEs, discontinuation, mortality, and new-onset diabetes; the HeFH data still flags diarrhea and dizziness as specific symptoms to ask about and monitor.
Tolerability Is Not A Vibe
Trial reports often use phrases like “well tolerated.” The phrase is not useless, but it should earn its keep. In this case, the low discontinuation rate due to adverse events supports it. So does the reported 97–98% adherence in CORALreef Lipids, which suggests that participants were generally able to keep taking the daily oral therapy during the trial period.[3]
Adherence is not the same as safety. A person can adhere to a medication while having mild symptoms, and adherence in a trial can be higher than in ordinary practice because participants are observed, reminded, and selected. Still, when adherence is near complete and AE-related discontinuation is low, it becomes harder to argue that tolerability problems were broadly limiting treatment in the trial.
The oral route also changes which adverse events you expect to see. Enlicitide avoids injection site reactions because it is not injected. That is a real practical difference from injectable PCSK9 inhibitors, where injection site reactions are a known issue, but it should not distract from the central safety reading task.[3] Route-of-administration advantages do not replace the trial-arm comparison.
Do Not Let Approval Answer The Safety Question For You
The FDA approval establishes that regulators judged the submitted evidence sufficient for the approved use.[4] It does not mean every safety question is finished. Approval and long-term certainty are different claims.
The current CORALreef safety interpretation is bounded by trial duration. The available trials followed participants over a 24- to 52-week window.[1][3] That is enough to detect common or moderately frequent tolerability problems during the study period. It is not enough to confidently exclude rare harms, late-emerging effects, or safety patterns that require broader real-world use.
The ongoing CORALreef Outcomes trial, identified as NCT06008756 and designed for more than 14,500 participants, is the kind of larger outcomes dataset that can better address lower-frequency and longer-term questions.[2] Until those data mature, the clean teaching conclusion should stay within the evidence: reassuring current trial safety, not settled lifetime safety.
A Student-Ready Reading Of Enlicitide Side Effects
If you had to turn the enlicitide safety data into a short clinical interpretation, it would sound like this: in CORALreef Lipids, adverse events were common but nearly balanced between enlicitide and placebo at 64% versus 62%; serious adverse events, discontinuation due to adverse events, mortality, and new-onset diabetes were also comparable between arms.[1] That pattern supports a favorable short- to mid-term tolerability profile in the studied population.
Then add the part that prevents overstatement: in the separate HeFH population, diarrhea and dizziness showed imbalances versus placebo and should be treated as the specific adverse reaction signals to notice.[2] The broader trial did not show a standout imbalanced adverse event, and the available follow-up does not settle rare or longer-term risks.
That is the habit worth carrying into the next safety table: read the denominator, read the comparator, separate any-AE noise from serious outcomes and discontinuations, and reserve the word “signal” for differences that actually separate from placebo.
Comments
Join the discussion with an anonymous comment.