Lessons from the Cyclospora Outbreak for Public Health Students
This case study examines the 2026 Cyclospora outbreak—the largest in U.S. history—to teach students how outbreak investigations unfold in real time, from surveillance signals to traceback, and what happens when public health systems are underfunded.
Updated:
A useful cyclospora outbreak case study for students does not begin with a neat definition. It begins with a counting problem. On July 14, 2026, CDC reported 1,645 confirmed domestically acquired cyclosporiasis cases across 34 states, including 141 hospitalizations, or 9%, and no deaths.[1] On the same day, Michigan was reporting 3,309 cases by itself, far above its usual roughly 50 cases in a year, while CDC’s Michigan count stood at 145.[2] That is not a typo to be corrected before class. It is the case.
The mismatch tells students something that a polished final outbreak report often hides: surveillance is a living system. State investigators may be seeing patients, lab reports, interviews, and local clusters before those records have moved through federal confirmation and reporting channels. In this outbreak, STAT reported a six-week lag between state and federal tallies.[2] So the simple classroom question, “How many cases are there?” becomes a methods question: which case definition, which reporting level, which date, and which bottleneck?
The line list is never as clean as the lecture slide
In an introductory outbreak investigation exercise, the first page usually hands students a tidy line list: onset date, age, county, symptoms, exposure, lab result. In July 2026, investigators had to build that list while the outbreak was still expanding, while federal counts lagged state counts, and while some infections were probably still invisible because the parasite requires the right diagnostic request.
Cyclospora is especially good at exposing weak spots in case finding. NPR reported that the parasite requires special stool testing and is not part of routine gastrointestinal panels.[3] Johns Hopkins Medicine describes the incubation period as about seven days and notes that the illness can cause prolonged watery diarrhea.[4] Each of those details changes the investigation. A longer incubation period stretches the exposure window. Prolonged symptoms may send people to care days after eating the implicated food. Special testing means a clinician can suspect “stomach bug,” order a routine panel, and still miss the organism.
That is why the first operational move is not “find the source.” It is “make the cases findable.” A working case definition has to specify the person, place, time, symptoms, and laboratory criteria clearly enough that local health departments can sort reports consistently. If it is too narrow, investigators miss real cases. If it is too broad, they flood the line list with unrelated diarrheal illness. In this outbreak, the state-federal discrepancy makes that balancing act visible. Michigan’s number and CDC’s number were not merely competing scoreboard entries; they reflected different points in the surveillance pipeline.[1][2]
| Student question | What the 2026 outbreak teaches |
|---|---|
| How many cases are there? | The answer depends on case definition, testing, reporting level, and reporting date. |
| Why not just test everyone with diarrhea? | Cyclospora requires special stool testing, so detection depends on clinical suspicion and lab capacity. |
| Why are interviews hard? | A roughly seven-day incubation period asks patients to remember meals from a longer exposure window. |
| Why can a traceback be persuasive but not final? | A lettuce supply chain can converge on one supplier while other vehicles remain under investigation. |
| Where does policy enter? | Surveillance requirements, staffing, and traceability systems affect speed and completeness. |
Signal detection starts before certainty
A multistate outbreak rarely announces itself as a multistate outbreak. It starts as local oddness: more reports than expected, a laboratory result that makes a nurse epidemiologist pause, several patients naming similar foods, or a county health department asking whether neighboring jurisdictions are seeing the same thing. Michigan’s 2026 numbers show why local and state work matters. A state that typically sees around 50 cases annually was reporting thousands by mid-July.[2] That kind of jump is not a subtle signal.
Still, a signal is not yet an explanation. Investigators need to know whether the apparent increase reflects true disease, increased testing, duplicate reports, a changed case definition, delayed batching of reports, or some mixture of these. Students sometimes hear “surveillance artifact” as a dismissal. It is not. It is one of the first possibilities an investigator must check before assigning a cause.
The 2026 outbreak was already unusually large by federal count, and the reconciled total was expected to grow. The CDC health advisory described 1,645 confirmed domestic cases in 34 states as of July 14, while STAT reported that the outbreak had topped the previous U.S. record of about 4,700 cases when state-level data were considered.[1][2] The careful wording matters. “Largest recorded” is a surveillance statement as much as a biological one. It depends on who was tested, who reported, and which records had reached which system by which date.
The case definition has to survive real patients
Once a signal looks real, investigators need a case definition that can travel. It must be usable by a clinician ordering tests, a local investigator calling a patient, a state epidemiologist merging reports, and a federal analyst comparing states. For Cyclospora, that definition cannot lean only on generic gastrointestinal symptoms. Watery diarrhea helps point the investigation, but it does not distinguish Cyclospora from many other causes of illness. Laboratory confirmation becomes important, and that returns the investigation to the special-testing problem.
The long incubation period also changes the interview. For a fast-onset illness, students may be able to focus on a meal from yesterday. With Cyclospora, the relevant meal may be about a week earlier.[4] A patient may have eaten restaurant food, bagged greens, fruit, leftovers, and workplace meals during that window. The interviewer’s job is not simply to ask, “Did you eat lettuce?” It is to reconstruct plausible exposures without teaching the patient the answer.
That distinction is worth underlining. If investigators overemphasize a suspected food too early, interviews can become contaminated by expectation. If they keep the questionnaire too broad for too long, they may miss the common exposure hiding inside ordinary eating habits. Good outbreak questionnaires are not just lists of foods. They are instruments for preserving memory, timing, and comparability under pressure.
Exposure histories turn scattered illness into testable hypotheses
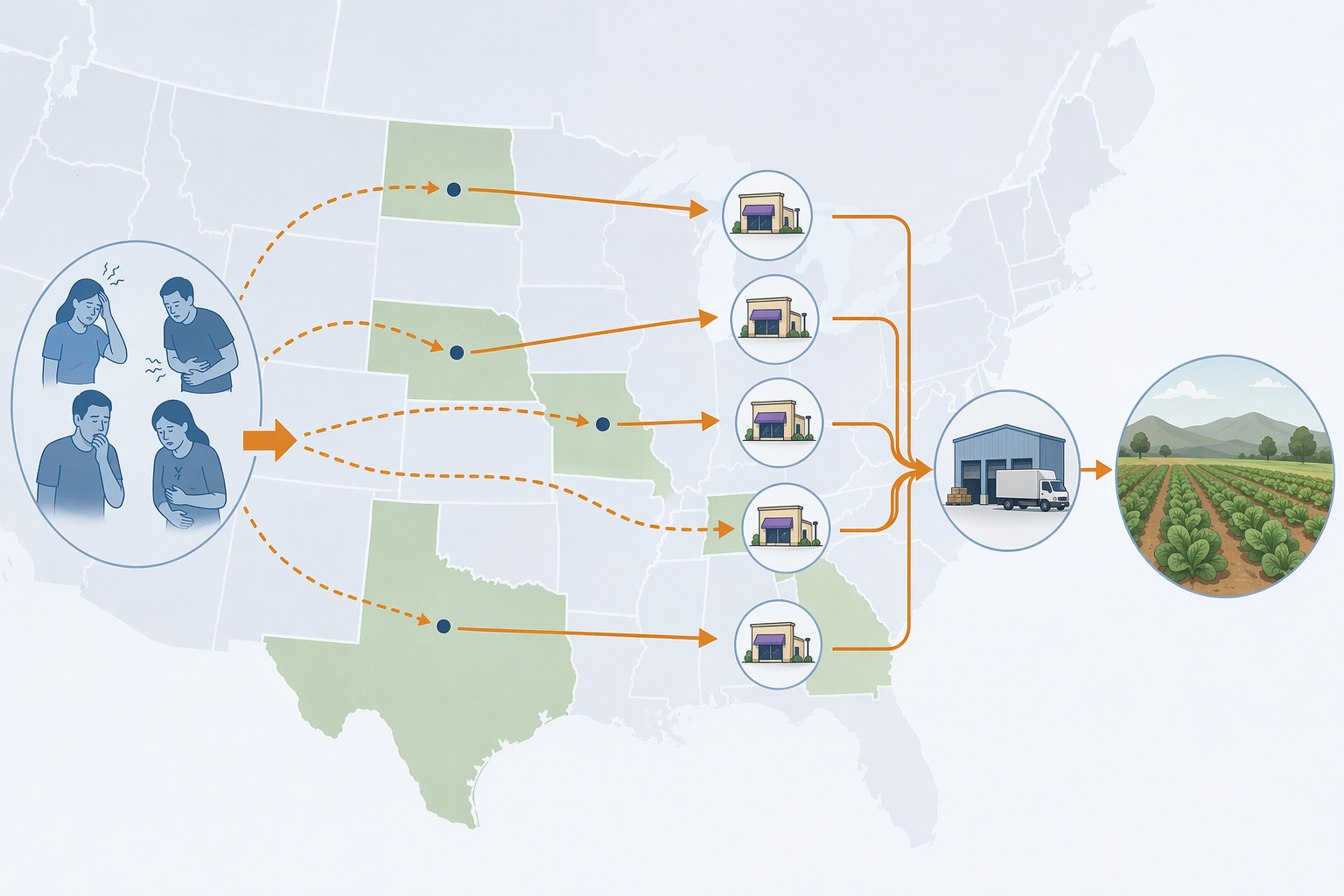
The food vehicle in the 2026 investigation points to shredded iceberg lettuce served at Taco Bell in five states, traced to a single Mexican supplier, according to CDC’s outbreak page.[5] Michigan officials had also identified lettuce or salad greens as an early signal.[5] For students, this is the moment when descriptive epidemiology begins to earn its keep. Person, place, and time are no longer boxes on a worksheet. They decide which exposures are plausible enough to investigate.
A restaurant-associated signal is helpful because it gives investigators a roster of possible menu items, purchase records, distribution pathways, and locations. It is also treacherous. Taco Bell customers may order multiple items. Shredded lettuce may appear across menu combinations. Some patients may not remember toppings. Others may remember the brand more clearly than the ingredients. A shared restaurant exposure narrows the field, but it does not by itself prove which ingredient carried the parasite.
This is where analytic epidemiology enters. Investigators can compare exposures among ill and non-ill people, or among people with confirmed cyclosporiasis and appropriate controls. They can ask whether illness is more common among people who ate items containing shredded iceberg lettuce than among those who ate otherwise similar meals without it. The answer is rarely as tidy as a classroom odds ratio suggests, because real menus share ingredients and real patients have imperfect recall. But the logic remains the same: a suspected exposure should explain the pattern better than competing explanations.
Traceback can strengthen a hypothesis without closing the case
Traceback is the part of foodborne investigation that students often imagine as a straight arrow from plate to farm. In practice, it is more like trying to redraw a supply chain from invoices, distribution records, delivery schedules, lot information, and product movement. The 2026 lettuce finding is powerful because shredded iceberg lettuce served at Taco Bell in five states was traced to a single Mexican supplier.[5] A common supplier gives the epidemiologic pattern a concrete route.
But a route is not the same thing as a complete account. The investigation remained active, and other food vehicles had not been definitively ruled out.[5] That caveat is not a legalistic footnote. It protects the integrity of the analysis. If students learn only to celebrate the moment a traceback points somewhere, they miss the harder question: does the traceback explain enough of the cases, across enough places and dates, to support action while uncertainty remains?
The single-supplier detail matters because it can connect geographically separated illnesses through a shared distribution pathway. The five-state Taco Bell detail matters because it gives investigators a bounded commercial setting in which to compare records. The early Michigan lettuce or salad-greens signal matters because it shows that local interviews were already producing a plausible food category before the full national picture settled.[5] None of those facts is sufficient alone. Together, they show how evidence accumulates across interviews, analysis, and records.
Policy pressure shows up inside the workflow
Funding and staffing are sometimes discussed as if they float above outbreak investigation. In this case, they belong inside the workflow. In July 2025, CDC’s FoodNet made Cyclospora surveillance optional, reducing the number of monitored pathogens from eight to two mandatory pathogens: Salmonella and Shiga toxin-producing E. coli.[6] That does not prove that the 2026 outbreak was detected late because of that specific change. The available evidence does not support that direct causal claim. It does, however, change what students should notice about resilience. Optional surveillance is different from routine, expected surveillance when a rare or under-tested pathogen starts moving through the population.
Staffing is the same kind of issue. The Guardian reported that more than 3,000 public health workers had left CDC through firings, forced retirements, and attrition before the outbreak, roughly a quarter of the agency’s workforce.[7] A number like that should not be used as a shortcut explanation for every delay or uncertainty in July 2026. It should be treated as capacity context. Someone still has to answer calls from states, harmonize case definitions, analyze exposure data, coordinate traceback, update advisories, and communicate uncertainty without getting ahead of the evidence.
The practical consequence is not abstract. If fewer people are available, or if surveillance is less systematic, the same classic steps become harder to execute quickly and consistently. A delayed interview can weaken recall. A delayed lab confirmation can slow case classification. A delayed federal reconciliation can leave students, reporters, and even practitioners comparing numbers that are true in their own systems but not directly interchangeable. The Michigan discrepancy is therefore not just a media oddity; it is a teaching specimen.
What students should practice with this case
A good case discussion should make students do more than repeat the suspected food vehicle. The useful work is to ask what each piece of evidence can and cannot support at a given point in time. The CDC count supports a confirmed multistate outbreak across 34 states as of July 14.[1] Michigan’s count supports a much larger state-recognized burden and a major reporting-timeline problem.[2] The lettuce traceback supports a strong food-vehicle hypothesis in five states, not a final explanation for every case.[5]
- Separate the date of illness onset from the date of diagnosis, report, confirmation, and federal posting.
- Ask whether a case count refers to confirmed cases, probable cases, state reports, or federal reports.
- Treat special stool testing as a surveillance filter, not a minor laboratory detail.
- Use incubation period to build the exposure window before narrowing the questionnaire too aggressively.
- Read traceback findings as evidence about supply chains, not as automatic proof that all cases share one vehicle.
- Keep policy variables close to the methods they affect: testing, reporting, interviewing, analysis, and coordination.
Consumer Reports’ proposed reforms—mandatory Cyclospora testing at import, restored surveillance funding, and better traceability systems—map directly onto those weak points.[8] Import testing concerns what is caught before food reaches consumers. Surveillance funding concerns whether unusual illness is detected and tracked. Traceability concerns how fast investigators can move from a menu item to a supplier and, if needed, farther upstream. Students do not have to agree on every policy prescription to see the operational target of each recommendation.
The unresolved ending is part of the lesson
As of Q3 2026, this outbreak does not offer the satisfaction of a completed final report. The final case count, complete traceback findings, and policy consequences may take weeks or months. That is uncomfortable for students who want outbreak investigation to behave like a solved problem set. It is also honest.
The 2026 Cyclospora outbreak shows that the classic tools still matter: notice the signal, define cases, obtain the right tests, interview carefully, compare exposures, trace the supply chain, and revise conclusions as evidence improves. It also shows that those tools are not self-executing. They depend on surveillance infrastructure, laboratory capacity, reporting timelines, staffing, and records good enough to follow food backward through a complicated system.
For a case discussion, the discipline is to keep uncertainty labeled. A moving outbreak can still be analyzed with care, provided students learn to ask what is known, how it was known, who has not reported yet, and what the system was built—or no longer built—to see.
References
- Health Alert Network (HAN) 00531, CDC, July 14, 2026.
- Cyclosporiasis outbreak cases top previous record of 4,700 cases, STAT News, July 14, 2026.
- Cyclosporiasis Cyclospora outbreak diarrhea states US, NPR, July 12, 2026.
- Cyclosporiasis Outbreak, Johns Hopkins Medicine.
- Cyclosporiasis Outbreak Investigation, July 2026, CDC.
- CDC cuts back foodborne illness surveillance program, CIDRAP, July 2025.
- Diarrhea outbreak Cyclospora parasite CDC, The Guardian, July 16, 2026.
- Cyclospora Outbreak 2026: What Consumers Need to Know, Consumer Reports, 2026.
Comments
Join the discussion with an anonymous comment.