A Medical Student's Guide to Lewy Body Dementia Symptoms
Master the 2017 DLB diagnostic criteria with a symptom-classification guide organized around core clinical features, biomarkers, and supportive findings — designed for rapid recall on boards and during clerkships.
Updated:
Lewy body dementia symptoms for medical students are easiest to learn when they are not treated as one long symptom list. The 2017 Dementia with Lewy Bodies Consortium criteria sort the findings by diagnostic weight: core clinical features, indicative biomarkers, supportive clinical features, and supportive biomarkers. That sorting is the difference between recognizing the disease and just remembering that “hallucinations plus parkinsonism” sounds familiar.
DLB matters because it is common enough to show up on exams and in clinic, but still missed in practice. StatPearls describes Lewy body dementia as accounting for up to 20–30% of dementia cases and as the third most common dementia category after Alzheimer disease and vascular dementia, while also emphasizing underdiagnosis and diagnostic delay.[1] For a student, the practical problem is that DLB can masquerade as Alzheimer disease, Parkinson disease dementia, delirium, depression, or a primary psychotic disorder unless the symptoms are sorted correctly.
If you are building this into your board-review system alongside resources like Anki vs Quizlet for Medical Students, make the diagnostic hierarchy the card structure. Do not make every symptom an equal bullet.
The 2017 DLB Scaffold
The first required clinical anchor is dementia: progressive cognitive decline that interferes with usual social or occupational function. Memory may be less prominent early than attention, executive function, and visuoperceptual impairment, which is one reason a DLB stem may not read like a classic Alzheimer disease stem at first pass.[2]
| Diagnostic bucket | What belongs there | How to use it |
|---|---|---|
| Core clinical features | Fluctuating cognition; recurrent well-formed visual hallucinations; REM sleep behavior disorder; spontaneous parkinsonism | These are the main symptom clues in stems and on clerkships |
| Indicative biomarkers | Reduced dopamine transporter uptake on SPECT/PET; low MIBG myocardial uptake; PSG-confirmed REM sleep without atonia | These can upgrade diagnostic confidence when paired with symptoms |
| Supportive clinical features | Severe antipsychotic sensitivity, autonomic dysfunction, falls, syncope, hyposmia, hypersomnia, mood and behavioral symptoms | These strengthen the pattern but do not carry the same diagnostic weight |
| Supportive biomarkers | Relative medial temporal lobe preservation on MRI; occipital hypometabolism on FDG-PET; posterior slow-wave activity on EEG | These are helpful reinforcers, especially in distinguishing DLB from Alzheimer disease |
The Four Core Clinical Features
The four core clinical features are the highest-yield symptom group: fluctuating cognition, recurrent visual hallucinations, REM sleep behavior disorder, and spontaneous parkinsonism. In a question stem, these may be scattered across family comments, sleep history, mental status changes, and the neurologic exam. Your job is to recognize which findings are core criteria and which are merely supportive noise.
Fluctuating cognition is delirium-like, not just forgetfulness
DLB fluctuations are spontaneous changes in cognition, attention, and arousal. The useful mental image is not a patient who misplaces keys more often over months. It is a patient who seems lucid in the morning, inattentive and drowsy later, then surprisingly engaged again without a clean metabolic or infectious explanation. The 2017 consensus report describes these fluctuations as typically delirium-like and notes wide prevalence estimates, ranging from 45% to 90% depending on how they are measured.[2]
That creates a real bedside trap. A fluctuating DLB patient can look “delirious,” and delirium still has to be considered. The clue is recurrence and spontaneity in the setting of progressive dementia and other DLB features. On exams, look for daytime drowsiness, staring spells, disorganized speech during episodes, or inconsistent attention that family members describe as part of the illness pattern rather than a single acute change.
Visual hallucinations are recurrent, well formed, and detailed
The visual hallucinations of DLB are not vague uneasiness or a patient saying the room feels strange. They are typically recurrent, well formed, and detailed: people, animals, children, figures in the room. The consensus report notes that visual hallucinations occur in up to 80% of patients with DLB.[2]
This is where a psychiatric framing can mislead. A late-life patient with detailed visual hallucinations plus cognitive decline deserves a neurologic differential, especially if the hallucinations appear with fluctuations, RBD, or parkinsonism. Auditory hallucinations, delusions, anxiety, depression, and apathy can occur, but recurrent well-formed visual hallucinations are the core feature to retrieve first.
REM sleep behavior disorder became a core feature in 2017
REM sleep behavior disorder is the one many students underweight because older teaching materials placed less emphasis on it. In the 2017 criteria, RBD was upgraded to a core clinical feature. The history is usually dream enactment: shouting, punching, kicking, falling out of bed, or injuring a bed partner during sleep. The key physiology is loss of normal REM atonia, which can be confirmed on polysomnography.[2]
The numbers make RBD worth remembering. The consensus report cites RBD in 76% of autopsy-confirmed DLB cases compared with 4% of non-DLB cases, and PSG-confirmed REM sleep without atonia is associated with a likelihood of synucleinopathy of at least 90%.[2] That does not mean every patient who acts out dreams has DLB, but it does mean that RBD plus cognitive decline is not a throwaway sleep-history detail.
Parkinsonism requires only one cardinal sign
Spontaneous parkinsonism is the fourth core clinical feature. For DLB criteria, only one cardinal feature is required: bradykinesia, rest tremor, or rigidity. The consensus report notes that parkinsonism eventually occurs in at least 85% of patients, but extrapyramidal signs may be absent early.[2]
Two exam traps sit here. First, do not require the full Parkinson disease picture before counting parkinsonism. Second, do not rule out DLB just because the early motor exam is not dramatic. A patient can have cognitive fluctuations and visual hallucinations before obvious rigidity or tremor becomes the feature everyone notices.
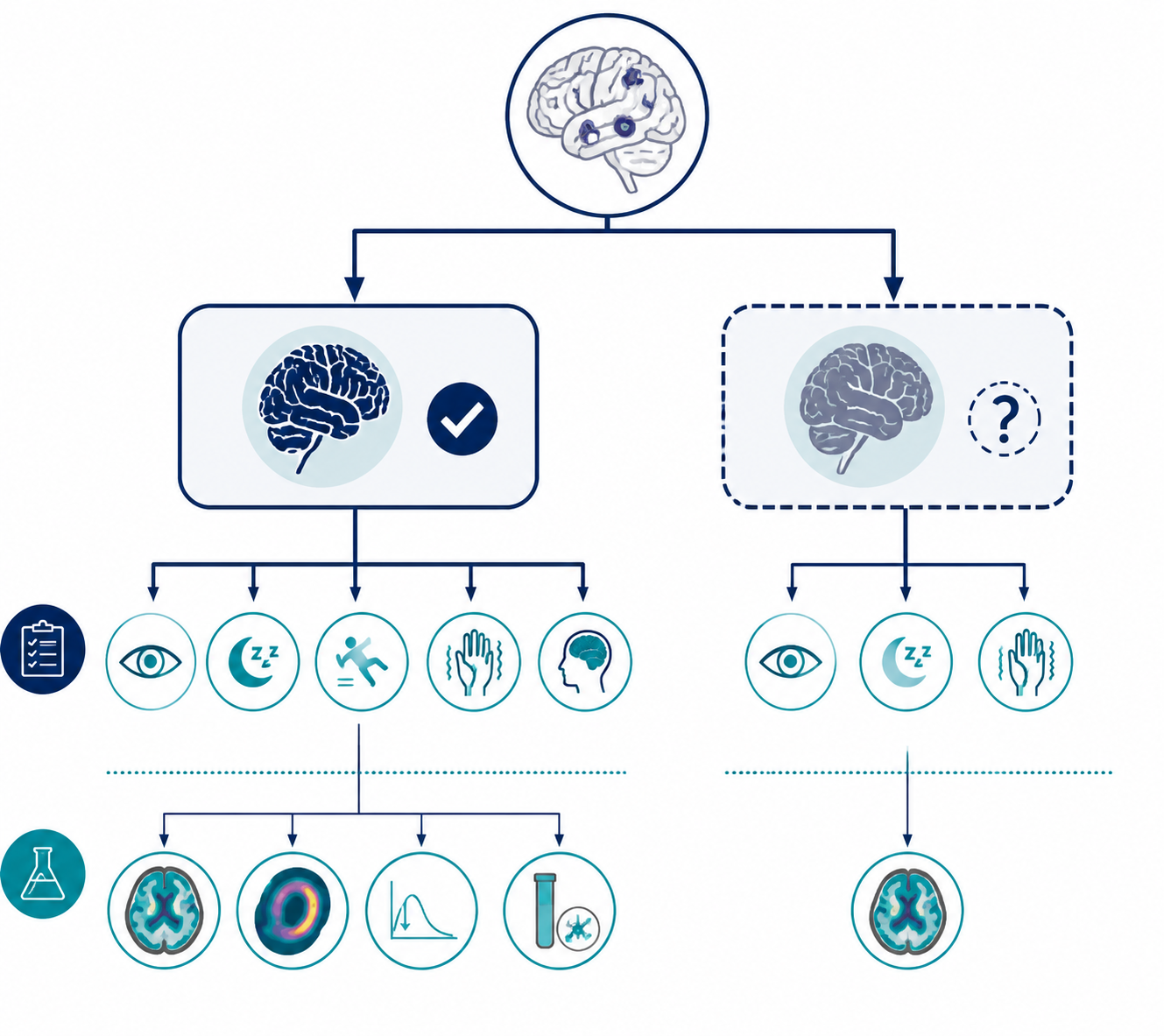
Probable vs Possible DLB
Once dementia is present, the 2017 criteria classify DLB by combining core clinical features with indicative biomarkers. This is the part to know cold for boards because a stem may give you one symptom and one test rather than two classic symptoms.
| Classification | Criteria |
|---|---|
| Probable DLB | Two or more core clinical features, with or without indicative biomarkers |
| Probable DLB | One core clinical feature plus one or more indicative biomarkers |
| Possible DLB | One core clinical feature without indicative biomarkers |
| Possible DLB | One or more indicative biomarkers without core clinical features |
Those combinations come directly from the fourth consensus report.[2] The important learning move is to avoid counting supportive features as if they were core features. Severe autonomic dysfunction, depression, and falls may support the diagnosis, but they do not substitute for a core clinical feature in the probable-versus-possible logic.
A board-style example can stay simple. A patient with progressive cognitive decline, recurrent detailed visual hallucinations, and dream enactment behavior has two core clinical features, so the presentation fits probable DLB even before imaging. A patient with dementia and only well-formed visual hallucinations fits possible DLB unless an indicative biomarker is also present. A patient with dementia, one core feature, and reduced DAT uptake moves into probable DLB.
Indicative Biomarkers Reinforce the Clinical Pattern
Indicative biomarkers are not random “extra tests.” In the 2017 criteria, they carry enough diagnostic weight to change possible DLB to probable DLB when paired with one core clinical feature, or to support possible DLB even when core features are not clearly documented.[2]
| Indicative biomarker | Board-relevant meaning |
|---|---|
| Reduced dopamine transporter uptake on SPECT/PET | Supports nigrostriatal dopaminergic degeneration; helps distinguish DLB from Alzheimer disease |
| Low MIBG myocardial uptake | Supports cardiac sympathetic denervation seen in Lewy body disease |
| PSG-confirmed REM sleep without atonia | Objectively confirms the physiology behind REM sleep behavior disorder |
Dopamine transporter imaging is the easiest biomarker to see in a test question because it connects directly to parkinsonism. The consensus report gives DAT SPECT/PET a sensitivity of 78% and specificity of 90% for distinguishing DLB from Alzheimer disease.[2] That specificity makes a reduced scan meaningful, but it does not turn the scan into a perfect rule-in/rule-out machine.
MIBG myocardial scintigraphy is also an indicative biomarker. The consensus report cites sensitivity of 77% and specificity of 94% in mild cases for distinguishing DLB from Alzheimer disease.[2] In U.S. student materials it may appear less often than DAT imaging, but in the criteria it is not a minor supportive clue.
Polysomnography-confirmed REM sleep without atonia is the third indicative biomarker. Clinically, the history may be enough to raise suspicion, but PSG confirmation gives the finding diagnostic weight as a biomarker. That distinction matters: “spouse reports dream enactment” is a core clinical feature when it supports RBD, while PSG-confirmed REM sleep without atonia is an indicative biomarker.[2]
Supportive Features: Pattern Recognition and Patient Safety
Supportive clinical features should not be memorized as a second equal list. They are useful because they make the whole picture safer and more recognizable, not because they independently establish probable DLB.
- Severe sensitivity to antipsychotic agents, which can be dangerous or potentially fatal
- Autonomic dysfunction, including orthostatic symptoms, constipation, or urinary problems
- Repeated falls or syncope
- Hyposmia or excessive daytime sleepiness
- Depression, anxiety, apathy, delusions, or other neuropsychiatric symptoms
Neuroleptic sensitivity deserves the most attention because it changes management. A patient with unrecognized DLB who is treated as having primary psychosis or agitation of nonspecific dementia may receive an antipsychotic and deteriorate. StatPearls, PsychDB, and Medscape all include neuroleptic sensitivity among the important supportive clinical features, and StatPearls emphasizes that antipsychotic sensitivity can be severe.[1][3][4]
For exams, that safety point often shows up as “worsening after haloperidol” or severe rigidity, confusion, or sedation after dopamine-blocking medication in an older patient with hallucinations and cognitive decline. The diagnosis is not just a label; it changes what drugs become risky.
Supportive Biomarkers Help Separate DLB From Alzheimer Disease
Supportive biomarkers carry less diagnostic weight than indicative biomarkers, but they can make a stem cleaner. The 2017 criteria list relative preservation of medial temporal lobe structures on CT or MRI, generalized low uptake on SPECT/PET perfusion or metabolism scans with reduced occipital activity, the FDG-PET cingulate island sign, and prominent posterior slow-wave activity on EEG with periodic fluctuations in the pre-alpha/theta range.[2]
The most useful contrast is with Alzheimer disease. Alzheimer disease classically leans harder on medial temporal atrophy, while DLB may show relative medial temporal preservation. Occipital hypometabolism can also point toward DLB rather than a straightforward Alzheimer pattern. These findings support the diagnosis; they do not replace the core clinical features and indicative biomarkers.
DLB vs Parkinson Disease Dementia: The 1-Year Rule
DLB and Parkinson disease dementia overlap because both sit in the Lewy body disease spectrum. The operational distinction is timing. If dementia occurs before or within 12 months of parkinsonism, classify it as DLB. If dementia develops after at least 12 months of established Parkinson disease, classify it as Parkinson disease dementia.[5]
That rule is practical, not a biological wall. Practical Neurology describes the 1-year rule as an operational convention rather than a biologically based distinction.[5] On exams, apply it because the test expects it. In real patients, use it without pretending the underlying disease processes are neatly separated.
Guardrails Against Overconfidence
DLB criteria are useful because they impose order, but the real disease does not always present as a clean checklist. Extrapyramidal features can be absent in up to 30% of cases, so a normal early motor exam does not eliminate DLB.[5] A normal DaTScan also does not fully exclude it; Practical Neurology notes that DaTScan can be normal in up to 20% of autopsy-confirmed DLB cases.[5]
Mixed pathology is another reason not to overread one clue. StatPearls reports Alzheimer disease co-pathology in 50–80% of DLB cases and notes that it predicts a more rapid course and worse global prognosis.[1] That helps explain why some patients look partly like Alzheimer disease and partly like DLB rather than matching a textbook category perfectly.
There is also an autopsy-level humility point: Practical Neurology notes that up to half of research-diagnosed Alzheimer disease patients have unsuspected Lewy-related pathology at autopsy.[5] For a student, the lesson is not to abandon the criteria. It is to use them carefully, know what each finding actually weighs, and avoid turning a probabilistic diagnosis into a brittle yes-or-no reflex.
The Rapid-Retrieval Version
Start with dementia. Then look for the four core clinical features: fluctuating cognition, recurrent well-formed visual hallucinations, REM sleep behavior disorder, and spontaneous parkinsonism. If there are two or more core features, think probable DLB. If there is one core feature, look for an indicative biomarker: reduced DAT uptake, low MIBG myocardial uptake, or PSG-confirmed REM sleep without atonia. One core feature plus one indicative biomarker also makes probable DLB. One core feature alone, or an indicative biomarker without core features, fits possible DLB.[2]
Then add the clerkship safety layer: ask about antipsychotic sensitivity, autonomic symptoms, falls, syncope, sleep, and mood. Use the 1-year rule to separate DLB from Parkinson disease dementia, but remember it is operational. Keep the caveats in your head: early parkinsonism can be subtle or absent, DaTScan can be normal, and Alzheimer co-pathology can blur the presentation.
References
- Lewy Body Dementia — NCBI Bookshelf.
- Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium — Neurology, 2017.
- Dementia with Lewy Bodies (DLB) — PsychDB.
- Dementia with Lewy Bodies Clinical Presentation — Medscape.
- Dementia with Lewy bodies: a practical guide to clinical diagnosis and management — Practical Neurology, 2026.
Comments
Join the discussion with an anonymous comment.