
Enlicitide Costs 35% Less Than Injectable PCSK9 Inhibitors at Launch
This comparison examines Merck's new oral PCSK9 inhibitor Lipfendra (enlicitide) against injectable PCSK9s and generic statins, showing that while enlicitide is the most affordable PCSK9 at $3,780/year, statins remain far cheaper, and real-world costs depend on insurance formulary placement.
Updated:
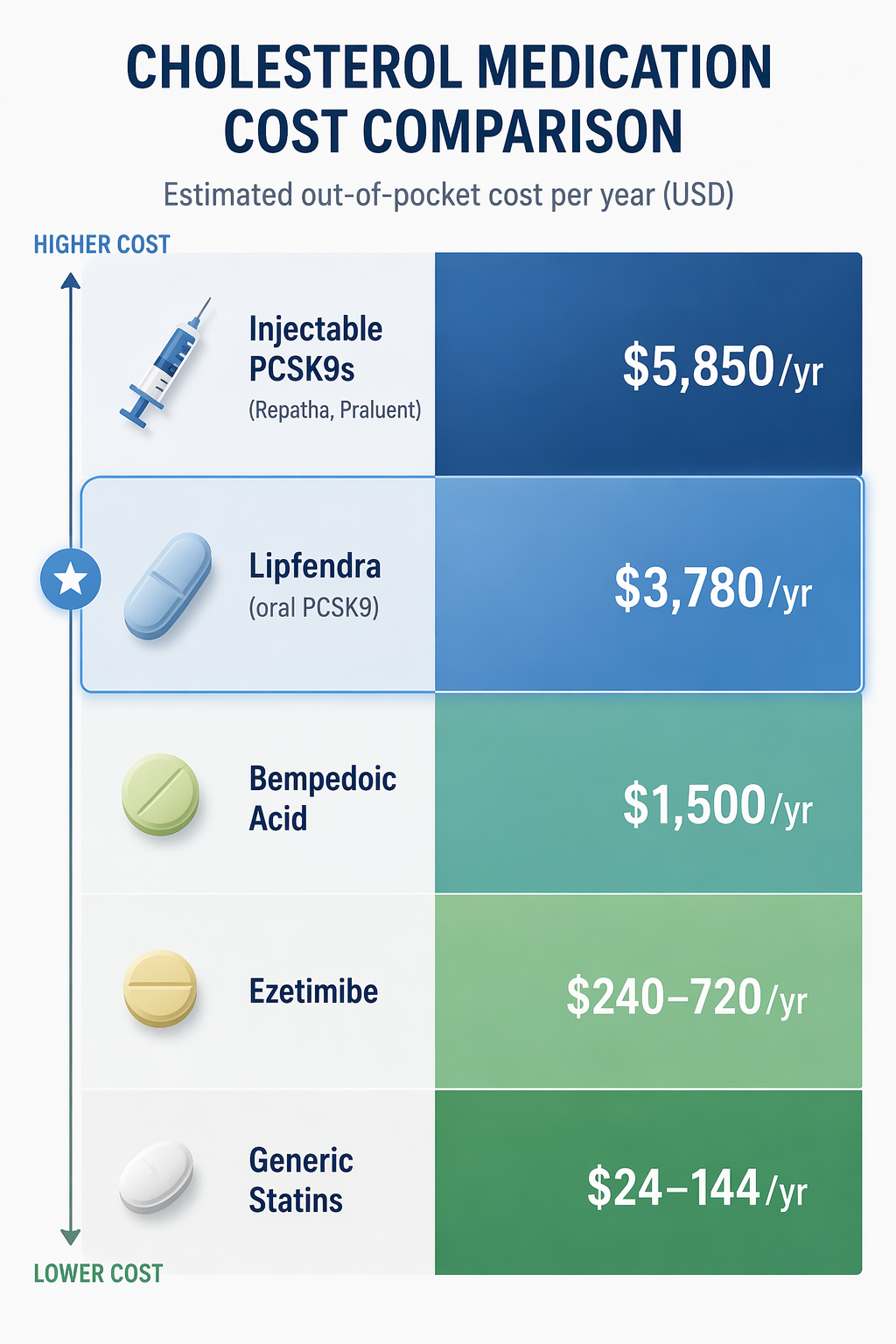
If Lipfendra, Merck’s enlicitide, is the first oral PCSK9 inhibitor, the first practical question is simple: is it actually cheaper than the shots? At launch, yes. Merck’s listed price is $3,780 per year, or $315 per month, compared with about $5,850 per year for the older injectable PCSK9 inhibitors Repatha and Praluent.[1] That makes Lipfendra roughly 35% cheaper than those injections on list price.
That answer needs a second sentence before anyone takes it to the pharmacy counter: Lipfendra is the cheapest PCSK9 inhibitor at launch, not the cheapest cholesterol drug. Generic high-intensity statins still sit in an entirely different cost category, roughly $24 to $144 per year.[1] A useful enlicitide cost comparison has to keep both truths visible, because “cheaper than Repatha” and “affordable for the patient in front of the pharmacist” are not the same claim.
The Cost Stack: Lipfendra Is Low for a PCSK9, High for a Pill
| Option | How it is taken | Price signal available now | What the number does and does not tell you |
|---|---|---|---|
| Generic high-intensity statins | Oral pills | About $24–144/year | Still the lowest-cost foundation therapy; not a PCSK9 inhibitor. |
| Ezetimibe | Oral pill | No verified price in the sources used here | Often considered before PCSK9 therapy, but this article does not have a verified dollar figure to compare. |
| Bempedoic acid | Oral pill | No verified price in the sources used here | A non-statin oral option; price and coverage can differ substantially from generic drugs. |
| Lipfendra (enlicitide) | Oral PCSK9 inhibitor | $3,780/year; $315/month list price | Lowest verified PCSK9 inhibitor launch price in this comparison. |
| Repatha / Praluent | Injectable PCSK9 inhibitors | About $5,850/year list price | The main benchmark for the 35% lower Lipfendra launch-price claim. |
| Leqvio | Injectable PCSK9-targeting therapy | No verified price in the sources used here | Relevant to the PCSK9 access conversation, but not part of the verified dollar comparison here. |
The clean comparison is between Lipfendra and the established self-injected PCSK9 drugs. On that measure, the new pill enters at a lower list price. The messier comparison is between Lipfendra and the sequence many patients already know: a generic statin, then perhaps ezetimibe, then another oral non-statin, and only later a PCSK9 drug if LDL-C remains too high or the patient is considered high risk.
That distinction matters because a $315 monthly list price may sound modest next to a specialty injection, yet still feel impossible to someone used to paying generic-drug prices. A plan that covers Lipfendra with a manageable copay could make it a serious access improvement. A plan that treats it as a non-preferred specialty drug could leave the list-price breakthrough mostly theoretical.
List Price, Cash Price, and Insured Cost Are Three Different Things
List price is the easiest number to compare because it is public and stable at launch. It is also the number least likely to match what an insured patient actually pays. For Lipfendra, the list price is $315 per month. That is the number behind the 35% lower-than-injectables claim.[1]
Cash-pay access is a separate pathway. Fierce Pharma reported that Lipfendra would be available through the TrumpRx direct-to-patient program, which could matter for people whose insurance denies coverage or creates delays.[2] The available sources do not verify comparable direct-pay monthly prices for Repatha or Praluent, so this comparison should not lean on forum-reported cash prices for those drugs as if they were confirmed market rates.
Insurance cost is the hardest number to know two days after approval. Lipfendra was FDA-approved on July 16, 2026, and formularies have not had time to settle.[2] A patient’s real bill will depend on whether the drug is covered, whether it lands on a preferred tier, whether a deductible applies, and whether the plan requires the patient to document prior use or failure of cheaper therapies.
Those categories should not be blended. A lower list price can help payers justify coverage. A cash program can help some people bypass a bad formulary. A preferred insured copay can make the drug usable month after month. They are related, but none substitutes for the others.
Why the $3,780 Price Is More Than a Marketing Number
There is a reason the launch price deserves attention even from people tired of hearing about “lower” drug prices that never show up at the counter. In a 2017 JAMA cost-effectiveness analysis, Kazi and colleagues estimated that PCSK9 inhibitor therapy would need to cost no more than $4,215 per year to meet a $100,000-per-quality-adjusted-life-year threshold in the modeled population.[3] Lipfendra’s $3,780 annual list price falls below that older threshold.
That does not prove every patient should use Lipfendra, and it does not prove insurers will cover it generously. Cost-effectiveness modeling is not the same as affordability at the pharmacy. But it does change the comparison. Earlier PCSK9 inhibitor prices were not just expensive in the ordinary sense; they were widely viewed as misaligned with value. Lipfendra enters closer to the range where the economic argument is no longer automatically upside down.
For a patient who has already used a statin, still has LDL-C above goal, and has been told a PCSK9 drug is clinically reasonable, that difference can matter. It gives physicians and patients a stronger argument when asking a plan to cover therapy. Whether the plan accepts that argument is the next, and usually more frustrating, question.
The Access Problem Lipfendra Still Has to Solve
The biggest warning sign in the PCSK9 market is not that the drugs do not lower LDL-C. It is that so few eligible people use them. Empirical Health cites an adoption gap of roughly 60,000 current US PCSK9 inhibitor users out of about 6 million eligible patients, or about 1%.[1] That is the number that should stay on the table when evaluating whether Lipfendra’s lower price will matter.
A lower launch price can remove one payer objection, but it does not automatically remove the paperwork. Plans may still require prior authorization. They may ask for LDL-C levels, diagnosis codes, proof of maximally tolerated statin therapy, documentation of ezetimibe use, or evidence that the patient fits a high-risk category. Some of those requirements may be clinically defensible. Some may simply slow people down until prescriptions are abandoned.
This is where patients often discover the difference between being “eligible” and being covered. A cardiologist can recommend a PCSK9 inhibitor. A trial can show LDL-C lowering. A manufacturer can set a lower price. The pharmacy counter still waits for the plan’s formulary decision, and sometimes for a reviewer who has never met the patient to decide whether the file is complete enough.
The early formulary questions are practical:
- Will Lipfendra be covered as a preferred PCSK9 option because its list price is lower?
- Will plans require patients to try Repatha or Praluent first, despite Lipfendra’s lower launch price?
- Will prior authorization rules mirror the older injectable PCSK9 process?
- Will cash-pay programs help patients whose plans deny coverage, or only a narrower group that can afford $315 per month?
- Will Medicare, commercial plans, and pharmacy benefit managers treat an oral PCSK9 differently from an injectable specialty drug?
Those answers will decide whether Lipfendra narrows the adoption gap or simply becomes another therapy that looks accessible in a headline and complicated in a benefits portal.
The Clinical Comparison Is Strong Enough to Take Seriously, but Not Finished
Lipfendra is not being compared with PCSK9 injections merely because it shares a category label. In the CORALreef AddOn trial, enlicitide lowered LDL-C by 60% when added to background therapy.[4] For patients and prescribers, that is the kind of LDL-C reduction that makes the cost comparison relevant rather than cosmetic.
The missing piece is long-term cardiovascular outcomes. The CORALreef Outcomes trial includes more than 14,500 patients and is still recruiting, with results expected in the 2027–2029 window.[1] Until those data are available, the economic case rests on LDL-C lowering, pricing, and existing assumptions about the relationship between LDL-C reduction and cardiovascular risk, not on completed event-reduction results for Lipfendra itself.
That is not unusual for lipid drugs at launch, but it should keep the verdict measured. A lower price and strong LDL-C lowering make Lipfendra a serious new option. They do not eliminate the need to see whether the pill ultimately reduces heart attacks, strokes, and other cardiovascular events at the expected scale.
The Pill Has Its Own Burden: Fasting
The word “oral” can make Lipfendra sound automatically easier than injections. For some people, it will be. Avoiding an injection pen is not a minor preference if it is the reason someone never starts therapy. But Lipfendra comes with an 8-hour fasting requirement, and that is not a trivial instruction in ordinary life.[1]
Trial adherence was high, at least 96% in the available data, but trial routines are not the same as rushed mornings, shift work, caregiving, travel, or multiple medications.[1] A pill that must be timed around fasting can still become a burden, especially for patients already managing diabetes, blood pressure drugs, or other daily therapies.
This affects cost in a practical way. A covered drug that a patient cannot take consistently may deliver less value than its price suggests. A more expensive injectable that a patient reliably uses may be the better fit for some people. The comparison is not just pill versus shot; it is the patient’s real routine versus the dosing rule.
So, Is Lipfendra Actually Cheaper?
On verified launch list price, Lipfendra is cheaper than Repatha and Praluent: $3,780 per year versus about $5,850 per year.[1] It also lands below the older JAMA cost-effectiveness threshold that has long framed the PCSK9 affordability debate.[3] For an oral PCSK9 inhibitor entering a market with very low adoption, that is real movement.
It is not cheaper than generic statins, and it is not automatically cheaper for every insured patient. The patient who most needs this information is often not choosing between list prices. They are waiting to learn whether their plan covers the drug, whether the copay is manageable, whether prior authorization is required, and whether the insurer accepts the medical history their doctor submits.
The fairest verdict is conditional. Lipfendra appears to be the most affordable PCSK9 inhibitor ever launched and may finally move PCSK9 therapy into a cost-effective price range. But most patients will not know their real cost until insurers publish formulary placement and prior-authorization rules. The list price makes the door easier to open; coverage decides whether most people can walk through it.
References
- Oral PCSK9 Inhibitor Lipfendra, Empirical Health.
- Merck scores FDA nod for Lipfendra, becomes first oral PCSK9 treatment, Fierce Pharma.
- Cost-effectiveness of PCSK9 Inhibitor Therapy in Patients With Heterozygous Familial Hypercholesterolemia or Atherosclerotic Cardiovascular Disease, JAMA, 2017.
- CORALreef AddOn trial, Journal of the American College of Cardiology.
Comments
Join the discussion with an anonymous comment.