
Cyclosporiasis Outbreak 2026: A Case Study for Medical Students
This case study uses the 2026 U.S. cyclosporiasis outbreak (1,645+ cases, Taco Bell/lettuce link) to teach medical students how foodborne outbreak investigations work — from case definition and FDA traceback to the clinical obligation to test and report.
Updated:
Last updated: July 18, 2026. The CDC case counts used here come from July 2026 updates, and this remains a live outbreak investigation. Numbers, state totals, and the strength of the food-vehicle link may change as surveillance reports and traceback work continue.
For medical students studying cyclosporiasis, the 2026 U.S. outbreak is useful because it does not sit neatly in one lecture category. It is epidemiology, food safety, clinical microbiology, and outpatient decision-making in the same case. As of July 16, 2026, CDC reported 1,645 laboratory-confirmed cyclosporiasis cases across 34 states, with 141 hospitalizations and no deaths; ages ranged from 2 to 95 years, the median age was 44, and 56% of patients were female.[1]
The signal was not just that cases existed. The signal was that they rose sharply. CDC’s Health Alert Network advisory reported 1,645 cases by mid-July compared with 249 cases during the same period in 2025, a 6.6-fold increase.[2] That is the moment when “summer diarrhea” stops being a vague seasonal complaint and starts becoming a surveillance problem.
CDC’s outbreak notice says epidemiologic and traceback evidence indicates that shredded iceberg lettuce served at Taco Bell locations was the likely source of illness in a multistate cluster, and FDA traceback identified lettuce from a single supplier in Mexico.[1] That wording matters. It supports a strong lettuce link, but it does not prove from the public-facing data exactly where contamination occurred in the chain, or whether cross-contamination happened during production, transport, distribution, or preparation.
The outbreak investigation chain, not just the headline
A foodborne outbreak investigation looks clean only after someone has written the final diagram. In real time, investigators begin with incomplete food histories, staggered symptom dates, different testing practices, and patients who may not remember which salad, garnish, or fast-food item they ate two weeks earlier. The 2026 outbreak is worth studying because it shows how several ordinary procedural steps can turn scattered cases into a usable public health signal.
| Investigation move | What it teaches |
|---|---|
| HAN advisory | A sharp rise over baseline can trigger clinician alerts before the investigation is closed.[2] |
| Local and state interviews | Food histories generate hypotheses, especially when many patients report overlapping restaurant or produce exposures. |
| Case definition and surveillance | A counted case depends on compatible illness, laboratory evidence, and reporting pathways. |
| FDA traceback | A suspected food vehicle is tested against supply-chain records rather than patient memory alone.[1] |
| Product identification and public communication | The public-facing message must be specific enough to act on while still preserving uncertainty where evidence is incomplete.[1] |
| Clinical testing and reporting | The outbreak remains undercounted if clinicians do not order Cyclospora-specific testing. |
The Health Alert Network advisory belongs near the beginning of the case because it shows how surveillance reaches clinicians. CDC did not simply announce an interesting parasite. It told health departments and clinicians that reported cyclosporiasis had increased substantially and asked them to consider testing patients with compatible illness, particularly during the usual May-to-August season.[2]
From there, the work becomes less glamorous and more important. State and local investigators interview patients, compare food exposures, and look for clustering by geography, time, and purchase location. In the Taco Bell-linked cluster, CDC reported that illness information and traceback evidence pointed to shredded iceberg lettuce served at Taco Bell restaurants in five states.[1] A named restaurant chain makes the case easier to remember, but the teaching point is the narrowing process: individual meals become exposure patterns, exposure patterns become traceback targets, and traceback targets become public health action.
That is also why the denominator is fragile. CDC’s confirmed count is not the same thing as the true number of infections. A patient has to seek care, the clinician has to suspect cyclosporiasis, the correct stool test has to be ordered, the laboratory has to detect and report it, and the report has to reach surveillance. One estimate places the true burden above 5,100 illnesses, but that should be read as an estimate of underdiagnosis pressure rather than as a firm CDC case count.
Michigan illustrates the reporting problem rather than resolving it. NPR reported more than 400 cases in Michigan in a cluster discussion, while also noting a Michigan-reported 2026 total of 3,309 cases, a figure that exceeds the national confirmed count described in CDC’s outbreak materials.[3] That discrepancy is not best treated as a mystery with a clean answer from the available sources. For students, it is a reminder that state and national counts may use different reporting windows, definitions, update schedules, or inclusion criteria.
How the lettuce link becomes more than a food-history coincidence
Food histories are noisy. Many people eat lettuce, and many people eat at chain restaurants. A single patient saying “I had tacos” does not identify a source. The useful signal appears when many cases share a specific exposure during a compatible time window, when the geography fits distribution records, and when traceback converges on the same product or supplier.
In this outbreak, CDC reported that epidemiologic and traceback evidence indicated shredded iceberg lettuce served at Taco Bell was the likely source for illnesses in the cluster under investigation, and that FDA traceback identified lettuce from a single supplier in Mexico.[1] The sentence is doing several jobs at once. “Epidemiologic” points to patient exposure patterns. “Traceback” points to supply-chain records. “Likely source” preserves the fact that public health conclusions often guide action before every mechanistic detail is known.
This is the part of outbreak investigation that medical students sometimes flatten into a memorized sequence: define cases, generate hypotheses, test hypotheses, conduct traceback. The sequence is correct, but it misses the practical hinge. The hypothesis only becomes useful when it is specific enough to test against records. “Fresh produce” is too broad. “Shredded iceberg lettuce served at certain Taco Bell locations, traced through supply records to a single supplier” is operational.
A brief historical comparison helps, but it should not take over the case. Cyclospora outbreaks have repeatedly involved fresh produce, which is why a lettuce-linked outbreak belongs in the mental neighborhood of prior produce-associated investigations rather than in the mental box of routine viral gastroenteritis. The 2026 value is that the chain is current and unusually visible: advisory, interviews, traceback, product identification, public updates, and clinical testing all sit in the same live investigation.
The clinical hinge: cyclosporiasis is missed unless someone asks for it
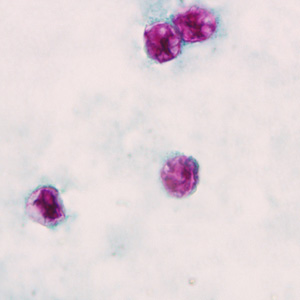
The bedside question is not “Can you recite Cyclospora cayetanensis?” The bedside question is whether a patient with prolonged or relapsing watery diarrhea in July gets the right diagnostic order. CDC describes cyclosporiasis as an intestinal illness caused by the parasite Cyclospora cayetanensis; symptoms can include watery diarrhea, anorexia, weight loss, cramping, bloating, nausea, fatigue, and low-grade fever, and untreated illness may persist for weeks or relapse.[4]
That symptom list overlaps with many outpatient complaints, which is exactly why the outbreak can be underdetected. A standard “stool O&P” order may not be enough. CDC’s clinical overview notes that Cyclospora testing must be specifically requested because the parasite is not routinely detected on all ova and parasite examinations.[4] CDC DPDx describes diagnostic approaches including modified acid-fast staining, ultraviolet fluorescence microscopy, and molecular methods such as PCR.[5]
Intermittent shedding adds another failure point. CDC DPDx notes that more than one stool specimen may be needed because oocyst shedding can be low or intermittent; when suspicion remains high, that can mean collecting three or more specimens at 2- to 3-day intervals.[5] That is not a test-taking detail. It changes what happens after the first negative result.
When to suspect it in clinic
- Watery diarrhea that is prolonged, relapsing, or not behaving like a short viral gastroenteritis.
- Illness during the typical late spring and summer cyclosporiasis season, especially May through August.[2]
- Recent exposure to fresh produce, salads, or advisory-linked restaurant items.
- Compatible symptoms during a known outbreak, even if the patient is not severely ill.
- A negative routine stool workup when the clinical course still fits cyclosporiasis.
For students preparing for rotations or USMLE-style infectious disease review, this is the kind of case worth putting into a spaced-repetition deck because the clinical action is attached to the epidemiology. A card that only says “Cyclospora causes watery diarrhea” is weaker than one that asks: “What stool tests should you request when Cyclospora is suspected during a summer produce-linked outbreak?” If you are building that workflow into your study system, an Anki medical-student review setup can help keep the diagnostic trigger attached to the testing order rather than floating as a fact.
Treatment is straightforward; recognition is the bottleneck
Treatment deserves clarity but not a pharmacology detour. CDC lists trimethoprim-sulfamethoxazole as the treatment of choice for cyclosporiasis, with the usual adult regimen of TMP-SMX 160/800 mg orally twice daily for 7 to 10 days.[6] The case does not become clinically useful unless the student connects that regimen to the earlier diagnostic decision.
| Clinical task | Practical action |
|---|---|
| First-line treatment | TMP-SMX 160/800 mg PO twice daily for 7-10 days.[6] |
| Sulfa allergy | CDC notes no highly effective alternative has been identified; ciprofloxacin has been used as a second-line option but appears less effective than TMP-SMX.[6] |
| Persistent suspicion after a negative test | Consider repeat stool specimens and verify that Cyclospora-specific testing was requested.[4][5] |
| Public health step | Report confirmed or suspected cases through local or state health department pathways. |
The hospitalization count gives the illness enough weight without overstating severity. CDC reported 141 hospitalizations among 1,645 confirmed cases, about 9%, and no deaths as of the July 16 update.[1] For most patients, the teaching issue is not mortality risk. It is prolonged morbidity, missed diagnosis, and the lost surveillance signal when cases never enter the reporting chain.
What students should watch agencies do next
A live outbreak is not a solved classroom vignette. Public health agencies may revise case counts, add or remove states, refine exposure windows, update product information, or clarify the distribution chain. The correct student posture is not to memorize one frozen number, but to notice what each update changes.
- If the case count rises, ask whether that reflects new illnesses, delayed reporting, expanded testing, or broader case definitions.
- If the implicated product changes, ask whether new traceback evidence replaced an earlier hypothesis or simply narrowed it.
- If a state total looks inconsistent with a national total, check reporting windows and definitions before treating it as a contradiction.
- If testing guidance is repeated in an advisory, assume underdiagnosis is part of the public health problem.
CDC’s older classroom cyclosporiasis case study remains a useful companion for practicing outbreak-investigation steps, but the 2026 outbreak adds the pressure of current clinical relevance.[7] It is one thing to solve a completed teaching case. It is another to recognize the same parasite in a patient still sitting in clinic while the advisory is active.
For students comparing study tools, this is also a good reminder that applied epidemiology is not learned only by reading lists of pathogens. A flashcard app comparison is useful only if the cards preserve the decision point: suspect Cyclospora, request the right test, treat when indicated, and report.
Where the student enters the outbreak
The public health machinery can detect a multistate rise, compare it with baseline, interview patients, trace lettuce through supply records, and warn clinicians. It still depends on the clinician at the front end of the diagnostic chain. During a summer outbreak, a patient with compatible gastrointestinal illness does not need a vague reassurance that “something is going around.” The patient needs someone to consider cyclosporiasis, order Cyclospora-specific stool testing, repeat specimens when suspicion remains, treat appropriately, and report through the right channel.
References
- CDC Cyclospora Outbreak Linked to Shredded Iceberg Lettuce at Taco Bell. CDC. July 16, 2026.
- CDC HAN Advisory HAN00531. CDC. July 14, 2026.
- NPR. NPR. July 12, 2026.
- CDC Clinical Overview of Cyclosporiasis. CDC.
- CDC DPDx — Cyclosporiasis. CDC.
- CDC Clinical Care of Cyclosporiasis. CDC.
- CDC Epidemiologic Case Study. CDC.
Comments
Join the discussion with an anonymous comment.